MUST-READ Selection(s):
'People Lose A Little Bit Of Weight'
So You Dislike The Prospect Of Civil War?


The content on this site is provided without any warranty, express or implied. All opinions expressed on this site are those of the author and may contain errors or omissions. For investment, legal or other professional advice specific to your situation contact a licensed professional in your jurisdiction.
NO MATERIAL HERE CONSTITUTES "INVESTMENT ADVICE" NOR IS IT A RECOMMENDATION TO BUY OR SELL ANY FINANCIAL INSTRUMENT, INCLUDING BUT NOT LIMITED TO STOCKS, OPTIONS, BONDS OR FUTURES.
Actions you undertake as a consequence of any analysis, opinion or advertisement on this site are your sole responsibility; author(s) may have positions in any firm or security discussed here, and have no duty to disclose same.
The Market Ticker content may be sent unmodified to lawmakers via print or electronic means or excerpted online for non-commercial purposes provided full attribution is given and the original article source is linked to. Please contact Karl Denninger for reprint permission in other media, to republish full articles, or for any commercial use (which includes any site where advertising is displayed.)
Submissions or tips on matters of economic or political interest may be sent "over the transom" to The Editor at any time. To be considered for publication your submission must be complete (NOT a "pitch"), include full and correct contact information and be related to an economic or political matter of the day. Pitch emails missing the above will be silently deleted. All submissions become the property of The Market Ticker.
Considering sending spam? Read this first.
The so-called "authorities" on health all admit that half of all adults are metabolically compromised (in terms of insulin resistance) with most of those over 65 being in this situation.
Being metabolically compromised places you at a materially higher risk of diabetes and heart disease. These are diseases that may kill you, but even if they don't they are debilitating. Obesity is a big part of that; you can't run, you can't move, you wind up with joint replacement surgery as you age (which has to be re-done every 10 or 20 years and is major surgery) and, if it gets out of control it can and will lead to amputations, blindness and ultimately kidney disease and dialysis.
This is a miserable way to live the last 20, 30 or 40 years of your life and it's not a pleasant way to die either.
Most people will say "well, I have no symptoms and my doctor is ok with what I'm doing", so they'll ignore the possibilities here. This is extraordinarily unwise as the damage that causes these diseases happens over years or even decades before clinical disease (that sends you to the doctor) presents itself.
It is easy and inexpensive, however, to know if that damage has accrued to the point that some detectable signs are present. You can do it at home, and you should because once these markers get into your medical chart they never go away and while people may think they're protected by Obamacare right now until and unless we deal with the medical monopoly situation in this nation you are risking financial ruin without cause if those markers get into your chart even if you reverse the damage.
What happened before Obamacare and will happen if and when it collapses? If those markers are in your chart you may become completely uninsurable at any rational cost. That means that any major medical emergency instantly bankrupts nearly anyone.
As an aside I'm going to make an assumption here: You're not diabetic today (diagnosed.) If you are diabetic then none of the below is news to you in terms of testing as you already have these results over time since they're part of what your doctor has you doing already. Nonetheless, you might be shocked at the improvement from the below eating pattern changes, so keep reading -- just ignore the testing thing, as you're already doing it.
This is something you can do in the privacy of your own home with nobody but you having the results. You can then change your behavior, specifically, what you do and do not eat, if you have a deteriorating situation and see if it improves. There is little cost to this, essentially zero risk over the time involved and if it doesn't work for you or if you think I'm a crackpot (I don't have an "MD" after my name, after all) you will have lost nothing other than a few dollars that were spent on something you probably ought to own anyway, one of which is not consumed.
You're going to go buy two things:
1. An A1c test kit. WalMart has them and they're under $30. There are two tests in the box, so each is about $15. No, one isn't for your SO, spouse or kid -- they're both for you. If you have two people to check buy two. These are consumed and tossed when used up.
2. An inexpensive glucose meter and a box of lancets. Buy one of the models with inexpensive strips; the meters are all cheap (~$20 or so) but the strip cost varies widely, by as much as 500%! While you're not using this for diabetes monitoring this is a device that will last years if not a decade or more so strip cost does matter, although not nearly as much. Again, WalMart has a wide selection -- IMHO make yours based on the strip cost (lower is better) and choose one that has individually-wrapped strips (this way they do not deteriorate by having a bulk package opened, since you are not using these multiple times a day as a diabetic would.)
When you get home open up the A1c kit, read the instructions (yes, you have to follow them to the letter to get good results) and run one. Keep the second. Write down the result.
The ADA and "some" docs say any A1c number under 6.0 is ok. You want a number at or under 5.6%. Note that these kits as with all tests, including lab tests, have an error band to them which means that one test provides decent information but you need to check it as the actual number could be a few tenths to either side of the displayed result. Don't use the second test immediately (unless the first errors out due to a mistake on your part); you'll use that a month or two down the road to both check the error band (the odds of a random error going the same way twice is 1 in 4 instead of 1 in 2) and your outcome.
Be aware that there are some confounding factors with the A1c test. First, it "assumes" blood cells live three months. We know this is not always true; people with severe metabolic damage tend to have them live for less (which means the number reads low) and those without said damage tend to have them live longer (which means the number reads high) since what A1c measures is the percentage of glycated hemoglobin in the blood. Further, if you have some conditions, among them anemia (in particular) it will read low because in that case hemoglobin is below normal levels -- this is a particular risk for women who don't get enough iron in their diet although there are other causes. This probably won't change your test result enough to matter, but it is the reason that standing alone an A1c test, while good and in fact an essential checkpoint, isn't enough.
Next, you're going to do two different checks with the glucose meter. The first is a fasting test, which is done when you first wake up in the morning before eating or drinking anything other than water. Most meters will store some amount of history but again, write it down. If your number is under 90 but greater than 50 that's ok. If it's under 50 test it again -- a persistent result under 50 is an indication of hypoglycemia (low sugar) which is dangerous as levels below 40 can cause you to pass out (and if nobody finds you and deals with it you can die), so if you get a confirmed reading under 50 consider obtaining medical advice. Again, the ADA and some docs say anything under 100 is ok. Correct clinically but wrong for the purpose you're intending here. If you get a number over 90 do it again the next day; if you get a second reading over 90 you've got a potential problem.
The final thing you're going to do is wait until you eat a "normal" meal at home (whatever that is) but it should include a decent amount of carbohydrate. "Decent" doesn't mean carb overload, but it does mean roughly the equivalent of one cup (cooked) of rice. If you eat low-carb normally, this is your chance to eat something you usually don't. Test your blood sugar level before eating, then test again both one and two hours after eating. Write down the results; no relying on memory here. You should not get a result over 140 on either of the post-eating tests and ideally within two hours you should be back to where you were before consuming the meal. If you're not, take a third test at the three-hour point.
Now let's interpret.
If you are eating food containing carbs on a regular basis, your A1c is at or under 5.6 and your fasting glucose is under 90, neither of the one and two-hour post-meal readings exceed 140 and you are back to baseline within three hours you are probably ok metabolically at this point. This doesn't mean you don't have insulin resistance of some amount but at this point it is not manifesting in clinically-detectable harm to your cardiovascular system. If you are eating low-carb and have been for several months or longer your fasting glucose level may be a few points higher, anything under 100, and is ok provided the other two tests are both in-range. Note that if you are overweight you probably are metabolically compromised (an OGTT w/insulin assay would easily detect it) but the test is expensive and frankly, the mirror works just as well for anyone in this category: If you have a gut, you're metabolically compromised. Incidentally just because you eat low-carb you are not necessarily going to get a somewhat-higher fasting glucose level; I don't, for example, and I've been eating low-carb now for something like five years now but some people do. If you are eating low-carb and get a reading over 90 for your fasting glucose there is a decent chance you're doing it wrong; specifically, you may be eating far too few green vegetables in an attempt to go "very low or zero carb" and thus massively short on vitamin and mineral nutrients. It is possible to eat "VLC" and not have this problem but severe nutrient deficiencies play hell with hormone levels, so don't just blindly accept that an elevated fasting level is "ok" -- it's not, and it usually means you're doing something wrong and accumulating damage.
If your A1c is over 5.6 (but under 6.0) or your fasting glucose is over 90 (over 100 for low-carb eaters) or your first two-hour post-meal readings (either or both of them) go over 140 or you are not back to baseline within 3 hours you are accumulating metabolic damage that is doing material harm to your body. Your doctor will probably not detect this in his routine screen but if you ran the (expensive) OGTT w/insulin assay test, which your insurance will not cover in this instance since there is no clinical indication of disease, I'll lay a large wager it would show significant metabolic compromise with insulin levels perhaps as much as twice normal levels. You're at severe risk down the road even if you are not overweight and if you are overweight you're a walking heart attack or stroke unless you change what you're doing. More than half of all adults in the US and most people over 65 are in this category or one of the worse ones below.
If your A1c is over 6% or fasting glucose is over 100 (irrespective of what you eat) or either of the first two post-meal readings is over 160 (you almost-certainly won't be back to baseline within 3 hours in this instance) you're either diabetic now or shortly will be. Your doctor will be able to detect this in a routine screen; if he's honest he'll call it "pre-diabetes" and if he does your medical chart will be "branded" forever which, to the extent legal now or ever again, will trash your ability to obtain health insurance at a rational cost. You'll also get a whole raft of pills shoved at you, probably including metformin (to start) and a statin. That's the traditional thing for them to do but it may be both harmful and unnecessary.
If your A1c is over 6.5% or fasting glucose is over 130 or any of your post-meal readings are over 200 you are in trouble as you are almost-certainly clinically diabetic now. This pretty-much meets the "bright line" test in the medical establishment to call you diabetic. If this is the case your chart and impact on health insurance is irrelevant if you change nothing as it is a virtual certainty you will if not are suffering real, material and serious damage to your health. You're probably symptomatic too but denying it. It is your call what to do with that information but before you run to the doctor for a formal diagnosis and permanent branding on your medical chart, assuming you haven't previously been diagnosed, read the rest of this article.
If you're of both of normal weight and your results are in the first category then relax -- and in a year, or if you become overweight, do it again just to keep tabs on things.
But let's assume you are either (1) overweight or (2) your results are in any of the bottom three categories irrespective of your weight.
Try the following for a short period of time (4 weeks):
1. Stop eating sugars of any sort. If it says "sugar", "fructose", "sucrose", "corn syrup", "hfcs" or anything of the sort anywhere on the label do not eat it. No more cookies, no more chocolate, no more sugar in the coffee, no sugared sodas, etc. Just stop. No exceptions, no tapering down, stop.
2. Stop eating starches and grains. No more pastas or potatoes of any sort. No more bread irrespective of the type.
3. Stop eating anything containing machine-processed vegetable oils. No more corn oil, canola, rapeseed, etc. No cooking with any of these oils and yes, that includes peanut oil; the only exception is olive oil as a salad dressing (e.g. with vinegar.) This crap is in a lot of "food" and no amount of it is healthy. This means no more packaged foods in the general sense; no more boxed dinners, canned ravioli, "lunch pouches or easy-prepare things" and similar (those probably break all three constraints!), nothing that comes in a bag (other than frozen vegetables), etc. This also means no fried food of any sort prepared away from home since essentially nowhere fries anything in either tallow or lard any more (but they should.) If you like wings find a place that bakes them and order them with the dry rub instead of the HFCS-laden sauce.
These three rules above are absolutes. You'll be tempted to cheat, but we're talking about a month here. Just don't; you can do it, and you know it.
Now on to what you do eat.
4. Do eat all the green vegetables, whole, not canned or packaged, you want. Find something or a bunch of somethings you like such as broccoli, brussels sprouts, bell peppers, lettuce and similar. Whole, fresh or frozen (e.g. in a bag) are fine; canned or otherwise processed are not. Substitute these any time you would otherwise eat any sort of snack and keep eating them until you're not hungry any more. It's not impossible and it won't hurt you; in fact, they're all good for you. It is close to impossible to overeat if you're consuming green vegetables.
5. Do eat full-fat protein. Pork, chicken (skin-on, not trimmed), steak, hamburger (no bun; that's grains), fish, eggs, cheese, etc. No restrictions on any of these foods, but eat when hungry until you're not, not until "full."
6. Use spices, including pepper, cumin, etc. as much as you wish. Hot sauces typically contain zero sugar and are perfectly fine even in wild amounts (yes, Tobasco is ok.) This is a taste-based thing, of course, but anyone who thinks you can't toss on the Lowrey's or pepper the hell out of your steak is flat-out wrong. Not only can you use salt unless you are one of a very small percentage of the population that has a genetic intolerance to sodium restricting salt intake is worse than worthless in that electrolyte imbalances lead to cramps (especially if you exercise) and can be dangerous.
7. Be careful with legumes and nuts. These are generally ok but nuts are very high in caloric content and it's easy to wind up eating 3,000 calories worth of them in a few minutes! So if you want a few as a snack, go ahead; just don't eat them as a meal rather than as a snack. But do not generalize this to nut-based oils (such as peanut oil) or anything processed from nuts because you are then concentrating the bad without the balance of the good (see above in point #3.)
8. If you normally consume alcoholic beverages keep it to one per day on average and not more than two on any day.
9. Drink any time you're thirsty; water is of course ok, if you like coffee go right ahead. Cream is ok (not non-dairy creamer, actual cream that has to be in the fridge) but sugar is not. If you want sweetener use any of the non-sugar ones (we're not going to be a nazi about these for this purpose.) Diet sodas may be ok, but if you can avoid them do so.
Do this for one full month.
Now repeat the above tests. Note that A1c typically measures average blood glucose levels over about a three month time frame, so the change there may not be dramatic and in addition the error rate on the test may obscure the results.
But remember the above table; if you drop a category or approach doing so you have hard proof that you required no medication whatsoever to improve your situation and these results are individual to you.
In other words you didn't read something on The Internet by some kook (like me), you didn't take blind advice from some doctor or nutritionist (irrespective of how many letters are after his name) you ran an individualized test with objective results on your particular genetic and metabolic make-up and have a set of numbers before you that document the outcome in your particular body.
If the results show no change (or get worse) then you've lost nothing other than a bit of time and a few dollars. Over this short of a period of time no harm is going to come to you; the harm that comes from bad metabolic markers in this regard requires years of accumulation before it "gets" you. But if the results are either dramatic or trend the right direction (and if you actually do the above it's a good bet they will) you now know that it is possible to change those objective metabolic markers through near zero-cost measures that are easily implemented in your daily life without spending one minute in a doctor's office or taking (and spending money on) one single pill.
Is that enough motivation to continue for another month or two and see if you can return your metabolic profile to the top, that is, "ok" category?
Further, you just prevented yourself from being "branded" in your medical chart and you didn't do it by cheating, you improved your actual metabolic profile.
That ought to be plenty of reason to continue on that path and make it a lifestyle, considering that the difference between said improvement to the top category and any of the others is a very material change in your risk of heart attack, stroke, blindness, amputation, dialysis and death! Further there's a very good chance that at the same time you're going to see a change on the scale if you're overweight, and I bet you'll like that change as well.
If this proves up it is going to be an absolute disaster for everyone in the health field -- in fact, it will be as bad as the disaster that resulted from exposure of the fact that leeches were worthless in "treating disease."
Coronary Artery Disease, or "CAD" for short, has proceeded from the following general premises:
1. Cholesterol in the blood binds to sites of inflammation in the artery, treating it much like it would a splinter in your foot.
2. That process is cumulative and, over time, blocks more and more of the artery.
3. Eventually this produces a blockage that either breaks off (a stroke) or you have a heart attack due to insufficient blood delivery to the heart muscle.
In fact if you look around Google for "Coronary Artery Blockage image" you will find hundreds of images that look like this:
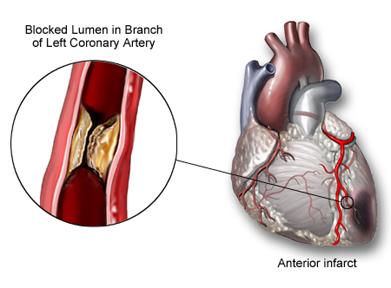
There's one problem -- they're all wrong.
The paper cited above points out the logical fallacies that have attached to the "common model" you're taught and that your doctor -- and cardiologist -- is using.
- This is a systemic disease, that is systemic inflammation is usually believed to be the root cause and it makes sense, except for one problem that this paper points out: The only place the arterial blockage tends to occur is in the cardiac arteries; the entire rest of the body appears to be either entirely unaffected or almost-entirely so. It is exceedingly improbable that systemic inflammation would leave all the other arteries in the body untouched yet selectively clog the ones around the heart. Indeed, every cardiologist knows this; where do you think they get arterial grafts from (usually veins in the leg) and how many of those do you think the average cardiologist has seen, and how many have asked "how come this one's not blocked too, given that it's a similar-sized blood vessel?"
- If high LDL-C levels produced CAD then removing the high LDL-C levels by any means (including drugs) would eliminate the disease. It does not; only about 30-40% of those at risk are "helped" and plenty of people with "normal" LDL-C levels get CAD. This means that the presence of LDL-C cannot be the cause of CAD since eliminating the presence of the alleged causative factor does not eliminate the disease.
- Invariably, as in the above image, the plaques are shown initiating at the arterial wall and growing inward. The problem is that this isn't what actually happens; the first depositions of LDL-C take place deep inside the arterial wall and there are few molecules present at the blood/wall boundary. This I was not aware of and you probably weren't either, given the above image that everyone has in their head that's ever looked at one along with the accompanying text. Guess what: That image and text is factually incorrect.
Now let's add some more facts to the mix that are discussed in the paper:
- The coronary arteries develop a multi-layer structure early in life through cellular differentiation that thickens until young adulthood, then stabilizes, maintaining itself thereafter. That is, this normal state develops in all humans over roughly the same time frame (immediate post-birth through age 30 or so.) Contrary to the common presentation the inner layer is not a single layer of cells; it is a multi-layer structure.
- There is a substance, proteogycan biglycan, that binds to LDL-C and is normally present in the outer layers of the coronary arterial wall. By contrast the inside layers are poor in this substance. However, the outer layers of the inside arterial wall cannot access LDL-C from the bloodstream flowing in the artery because the arterial wall is normally not vascularized -- that is, there are no capillaries bringing blood to it. Instead, oxygen and glucose reach these cells via direct diffusion. LDL-C is too large to diffuse through that distance in any material quantity irrespective of its presence in the blood.
- LDL-C does not accumulate starting at the inside arterial wall outwards. This effectively demolishes the claim that it is via the blood flowing in the artery and diffusion that such deposits are picked up and accumulate; it is logically inconsistent since to reach those outer layers the inner ones must be reached first!
- It is known that one of the reactions to oxygen starvation of cells is to stimulate vascularization. That is, when cell layers get too thick for diffusion to work any more they stimulate the development of capillaries to bring them oxygen and transport both glucose and waste.
- The appearance of vascularization always precedes the development of CAD and originates not from inside the inner arterial wall but rather from the outside in; in arteries where it is not present no plaque development occurs.
- This abnormal vascularization and concentration of LDL-C are observed in other tissues. Specifically, this has been observed in the cornea which is also normally not vascularized but, if it becomes so, fatty plaque formation occurs. This has been known for 50 years and yet has been ignored in the CAD "debate."
- Arterial plaques in the coronary arteries are more common in herbivores than carnivores, and occur in all eutherian (placenta-bearing) animals with a body mass comparable to or larger than humans. You've been told that CAD is a uniquely-human disease and meat-eating is more-dangerous in this regard than veganism. The claim that CAD is a human disease is a bald and knowing lie, and further herbivores are more susceptible to the disease than carnivorous eaters! So much for vegetarianism being protective against heart disease.
This paper roundly demolishes a number of claims that are made every day in the media and the medical establishment, and what's worse is that it completely decimates the balance of benefit and harm argument for the use of drugs to "lower cholesterol" such as statins because once the inner coronary arterial wall has become vascularized LDL-C will inevitably be picked up and accumulated.
Let's put forth what is directly attacked and, if this paper holds up, refuted:
- Coronary Artery Disease is a human condition. False; it is found in all placenta-bearing mammals of human or larger size.
- Coronary Artery Disease is a condition that is more-common and more-severe (or even exclusively present) in meat-eating animals. False; it is in fact more-common in herbivores than carnivores. That is, there is zero evidence that vegetarian eating is helpful and in fact the evidence among animals in general goes the other way.
- Coronary Artery Disease is caused by LDL-C. False; greatly attenuating LDL-C does not prevent the disease; it is at best 30-40% effective.
- Coronary Artery Disease begins with LDL-C carried in the arterial blood that diffuses through the inner arterial endothelium directly. Not likely; that is not a single-cell layer as commonly depicted, and the concentration of LDL-C is higher in the deeper layers, which is logically inconsistent with that claim. Further, CAD does not present in arteries that have not had the deeper layers vascularized which is logically inconsistent with the theory that LDL-C in the arterial blood deposits on or diffuses through the arterial wall.
The problem with what's presented here, from a medical perspective, is that if this paper proves up it doesn't leave you with a trillion dollar industry you can force people to spend money on by scaring them to death.
If in fact the growth of the inside layer of your coronary arteries in thickness is a risk factor that simply comes with time on the planet then given the inherent response of cells that become less-than-well supplied by oxygen (that is, to stimulate vascularization) there may be no actual cure available for this condition; it may simply be inherent in getting older, with some people more susceptible than others.
If, on the other hand, there is some sort of systemic insult responsible for the thickening of these inside walls beyond the limits of diffusion to provide transport that might be able to be addressed. The problem with such a belief is that you then have to find the same insult pathway -- whether from the same cause or not -- in the other mammals that also suffer from the condition. That becomes a rather serious problem since obviously other large placental mammals don't eat trans-fats or refined sugars, as just one example.
In short while this paper is a not a smoking gun as to cause it refutes a lot of false claims about coronary arterial disease and, if it holds up to scrutiny you may be witnessing the imminent destruction of a trillion-dollar a year scam.
Stay tuned.
PS: This paper's description is also consistent with why smoking promotes (but does not cause) coronary artery disease. Smoking raises CoHb levels, which in turn would tend to lead to cellular hypoxia, with the most-severe effects being in cells where the diffusion path is the longest. That, in turn, would be expected to promote vascularization..... Likewise, it explains the association between sleep apnea where depression of oxygen saturation has been documented and CAD -- an association that has been shown but I've yet to see a plausible scientific explanation as to why they're associated. This definitely appears to merit further study!
If you "diet" you will fail. You will fail because you never changed anything in the long term, and as soon as you go back to what you were doing the same result will come. What else can you reasonably expect?
If you have been reading the newspaper recently, you will have come across some startling new nutrition advice. A much hyped new study, conducted with just 150 participants, calls for us to “embrace fat”—even the saturated kind. The alleged benefits? Weight loss and, most incredibly, healthier hearts.
No kidding? Well, he thinks it is kidding.
In the two centuries during which these diets have been promoted, there have been hundreds of studies comparing low-carb to low-fat diets. One would think that by now it would be clear which was superior if there really was a difference. But if you take all of these diet studies, and analyze the enormous body of data they produced, there is no proven difference between them as far as weight loss is concerned. In fact, another such analysis was published the day after the over-hyped low-carb study with this same conclusion.
If you're looking for a diet, that is, something faddish you can do that will produce result "X", you can find it whether it's straight starvation or something else. Then there's this:
More to the point, however, is that this most recent study really did not actually prove that low-carb diets are superior. The low-fat diet in the study was not that low in fat, and the low-carb group ate significantly fewer calories.
Well duh.
See, people keep missing this -- it's a lifestyle choice, not a diet.
Do you eat fewer calories? Yes. You want to know why? Because you're not hungry, that's why.
There's no magic to it. When you're hungry if there is food available you'll eat, all things being equal. Oh sure, you can apply extreme willpower to counteract that, but will you succeed? Probably not at all, and almost-certainly not for long.
So what's the secret? It's easy -- don't be hungry.
That's what low-carb does, you see.
Sugars and things that quickly convert to sugar produce a "high." Ask any parent about their kid being jacked up on sugary things. Well if you've all seen this why do you think it doesn't happen to you?
And what comes after that when you "come down"? The crash, of course, and what do you want? More of what made you high.
Is it really any more difficult to understand than that?
Nope.
I'm going to be really rude this morning because frankly I've seen too much BS in the comments section and elsewhere to keep my mouth shut or be nice in response any more.
Notice that it says exactly nothing about the form or type of exercise you engage in (or don't), nor does it say anything about trying to set personal records in how much you (over)pay for various forms of food, most-particularly playing the so-called "organic", "free-range" or any other sort of horsecrap game in your infantile attempt to play "more expensive is better."
I refused to approve a few comments on that article, and ones before it, which boiled down to "watch me show you how rich I am because I paid $6/dz for eggs so they'd have a magic label on the package."
Might there be some further, small and incremental benefit from that? Maybe. But the point here is further, small and incremental.
I argue that this sort of crap is in fact destructive to the larger issue in that by strutting around showing off your wallet size you are providing a disincentive to millions of Americans by, in effect, claiming that unless you're rich you can't afford to quit stuffing your pie hole with crap.
That's a lie, by the way and to the extent you run it in public you ought to be called on it and shunned.
Oh I'm sure I'll get hate mail for this column, but I'm used to it. If it gets one person who thinks they have to buy $6/dz eggs in order to change their life when the $1.99/dz ones will do just as well along with the mass-produced Kraft brick cheese and mass-produced salted butter in their omelette at less than half the cost, when the alternative was a breakfast full of cereal and other garbage, then it's been worth it.
My refrigerator has mass-market eggs, butter and cheese in it for said omelette. I can afford the $6 eggs but I refuse to pay three times the price for something that might have tiny incremental benefits when I can get 80% or more of the benefit with the $2 eggs.
You folks arguing for the "organic" nonsense, in my experience, nearly all wind up destroying the benefit you would get from that 80% by eating other trash, but still think you're doing good. Rather than nuke some mass-produced and frozen brussel sprouts with mass-produced salted butter for lunch you instead have a "whole wheat" sandwich and suck up enough refined carbs to spike your insulin levels, utterly destroying any benefit in terms of body weight control and health you could have gotten from the eggs!
You pat yourself on the back but obtain nothing beyond a lighter wallet and another peacock feather that you then dutifully stick in your asshole and parade around showing off.
Sorry folks, no $ale. The simple fact of the matter is that 80% of the solution to nearly any problem can be had at reasonable cost provided you don't go ape-shit trying to play this sort of game. Arguing that people ought to blow money most of the population does not have on trying to achieve the last 20% before expending the effort and time, at much lower cost, to get the 80% solution taken care of is not only stupid it's actively destructive.
Feel free to do that on your own time and space, but around here if you get obnoxious enough about it I'll be happy to hammer you with this:
Yes, that's a 30 second Photoshop hack job. And?
This sort of horsecrap feel-good garbage ought to piss you off.
Especially in this case because if you believe it that act of stupidity may kill you.
There's a disturbing truth that is emerging from the science of obesity. After years of study, it's becoming apparent that it's nearly impossible to permanently lose weight.
....
We all think we know someone in that rare group. They become the legends — the friend of a friend, the brother-in-law, the neighbour — the ones who really did it.
But if we check back after five or 10 years, there's a good chance they will have put the weight back on.
Well yeah, if they don't change what they eat.
That's because obesity is mostly about what goes down your pie hole -- not how much goes down your pie hole.
In March of 2011 I got tired of being a fat bastard. I massed 210 lbs at that time and was uncomfortable in a 34" pair of jeans; 36s were ok. I wore an XL T-shirt or sweatshirt and filled them "amply." I was headed for 38s and then 40s on the jeans -- I'm sure of it. Oh sure, maybe not for another 5 or 10 years, but that's where I was headed and I knew it. I couldn't see my dick in the shower in the morning unless I sucked in my gut.
About nine months later I massed 150lbs -- a net 60 pound loss. I have been between 145 and 155 since with very few excursions to either extreme. Before writing this I stepped on the scale and it read 151. I do not count calories. I do run and bicycle, and did so while losing the weight, but I'm not obsessive about it. There are weeks I don't run at all, or run about a single 5k in distance. Then there are weeks I run pretty close to a 5k a day, or bike through an equivalent amount of time (and caloric consumption.)
When I began fewer than 10 flights of stairs would kick my ass. Today that would be no problem at all. A 5k run was literally impossible; I could not run for more than about a quarter of a mile at a time without having to slow down and feeling like I'd been hit by the truck.
My personal best today on a 5k is a 7:06 pace across the race and my "normal" pace while "having fun" is right around 8 minutes/mile. And I'm not a kid any more either -- I've got half a century on my sack of meat thus far.
I've posted this picture before. It's real.
If you think I'm funnin' you on my ability to maintain that over this period of time here's a "selfie" from a few minutes ago:
I have on a pair of 30" waist shorts and that's a size medium T-shirt -- the same size I've worn since late 2011. It is now June of 2014.
Oh, by the way, this isn't the first time I tried to lose the weight. I had previously failed several times, despite really working at it from a physical activity perspective.
What changed this time around?
I changed what -- not how much -- went in the pie hole.
Specifically, I got rid of most carbohydrates and grains, including all fast carbohydrates such as sugars and breads.
Today I keep it under 100g/day, am usually under 50g, and have frequent days during which I consume zero carbohydrate.
My body and metabolism reacted to that; after a relatively modest period of time I wasn't hungry very often, and thus I ate less, with the largest component of my caloric content shifting to saturated fat. I didn't have to try to eat less, I simply wanted less. Today I wake up and am often not hungry at all and may not have anything to eat until the middle of the morning or even later.
Then I'll make up some eggs cooked in butter with bacon or eat a steak, pork chop, chicken, ham and the like with utterly no attempt to reduce saturated fat intake at all. What I did eliminate in the "fats" department were vegetable and hydrogenated fats, with the exception of olive oil that I do use for cooking purposes and as a salad dressing.
Look folks, you can believe what you want. But the fact of the matter is that in my experience fast carbs are an addictive drug.
Like most addictive drugs they make you feel good but do bad things to your body.
Like most addictive drugs there are people who "push" them, but since these addictive drugs are legal there are a lot of people manufacturing and pushing them.
Let me give you an example. I used to like chocolate bars. I'd eat half a Snickers bar and if there was another half in a short while I'd want to eat that too. Then there better not be any more of them in the house or they'd be gone as well. The same with a bag of Doritos. Sure, a "serving" is a handful of chips. How many of you will eat those, then a while later consume the rest of the bag?
Doesn't that sound like addictive behavior? It sure does -- and I assert that's because it is.
Once you become fat through this addictive process you have a further problem -- not only are you habituated to these substances but in addition your insulin response mechanism is likely damaged. If that goes far enough we call it diabetes and if not controlled it will eventually cause you to get your extremities amputated, will make you go blind, and will eventually kill you.
Once you get diabetes you go to the doctor and they start prescribing medication. But if you keep eating carbohydrates -- that is, you keep using the drug that caused the damage in the first place -- drugs will become less and less effective because you are still doing incremental damage.
In many cases if you stop that crap your body can repair some of the damage over time. Not all of it, to be sure, and maybe not enough of it. But this much is certain -- if you keep doing damage the cumulative effect will continue to add up.
Our biology taunts us, by making short-term weight loss fairly easy. But the weight creeps back, usually after about a year, and it keeps coming back until the original weight is regained or worse.
That's like saying that the meth-head who has his teeth start to rot out, and who stops using it, ought to be surprised if his teeth keep rotting out if he goes back to smoking his crank-pipe!
Well, duh.
You can keep reading articles like this and nodding as you maw down on the Doritos and donuts or you can cut that crap out and do what I did.
Ultimately the problem is that it's hard to break the addiction, just like it is with all addictions. When you begin you crave these sorts of foods and if you succumb then you will fail. You'll then argue that it doesn't work when in fact you didn't maintain the path for long enough for the cravings to abate -- you cheated, in short, and after a period of time you'll declare failure and back to being fat you will go.
That's ok -- it's a choice, and one you're entitled to make. It's your ass -- literally, the size of your ass.
But do remember this -- today we have a medical system that is siphoning off 20% of our economy, roughly, and is running costs at 5x what they should be. It's a scam end-to-end, and will continue to be a scam because we refuse to put a stop to it by enforcing anti-trust law in this area just like we do and should everywhere else. There are a million excuses, just like there are a million excuses for the baked goods section in your grocery and the box of donuts on your kitchen table.
When -- not if -- that system comes unwound you will either have resolved this problem or you will have not. If you have you'll be fine because you won't have a diabetes problem and you won't need constant medical attention.
If not you will die.
Your choice, your consequence.